

Strollers

What to think about when determining the appropriate stroller for your child
Strollers and any type of manual wheelchair (WC) are considered the same when getting billed under insurance. If you chose to get a stroller, it is expected that it will last the child 5 years just as a manual wheelchair would.
Stroller vs. manual wheelchair (what insurance is looking for):
Manual wheelchairs allow for more adjustments and can grow with the child; therefore, if the child “seems” like they might need a wheelchair in the coming years, insurance will question whether the stroller is the most appropriate.
Strollers do not provide as many seating and positioning options:
Does the child require assistance to maintain upright sitting?
If the child requires lateral support at the trunk and/or hips then a WC might be more appropriate
Does the child have any spinal abnormalities or at risk for the development of scoliosis?
If yes, a WC might be more appropriate because of the added positioning options. Even if not needed now… additional positioning may be needed in the next 5 years.
Does the child have increased tone or spasticity causing their knees to come together, knees to extend out or head and trunk to thrust backwards?
If so, a WC can offer multiple accessories to assist in seating and positioning help minimize these motions that a stroller cannot provide.
How much time in this device during the day?
Will they be using it in school, during classroom activities, at home to accomplish tasks and school work, as a place to rest after a long day?
If yes, a WC might be more appropriate as it allows more upright sitting posture, more support if needed, can be positioned at a desk or table which will allow the child to better interact with their peers.
Is the child capable of propelling a wheelchair?
Strollers do not allow children to be independent with their mobility. If a child is going to be using the wheelchair while at school and at home and they ARE capable of propelling a WC, wheelchairs make children more INDEPENDENT; therefore, a WC is preferred.
What is the child’s potential for ambulation?
If the child is able to ambulate short distances, they will not need a device throughout the school day or to be used that majority of the day, then a stroller may be a good option.
If the child does not ambulate or ambulates short distances with or without a device, fatigues quickly, complains of LE or back pain with ambulation, fatigues quickly and is less active and has more trouble getting around at the end of the day, then a WC might be more appropriate.
If the prognosis for ambulation is unknown, take into consideration the other factors listed above to help determine what is best for the child NOW.
1. Sitting balance
2. Head and trunk control
3. Spinal abnormalities
4. Tone and spasticity
5. How often will this device be used
6. Can they sit in a standard chair at school or will they require more support throughout the day
7. Do they have good control and functionality of their upper extremities where they could propel a wheelchair
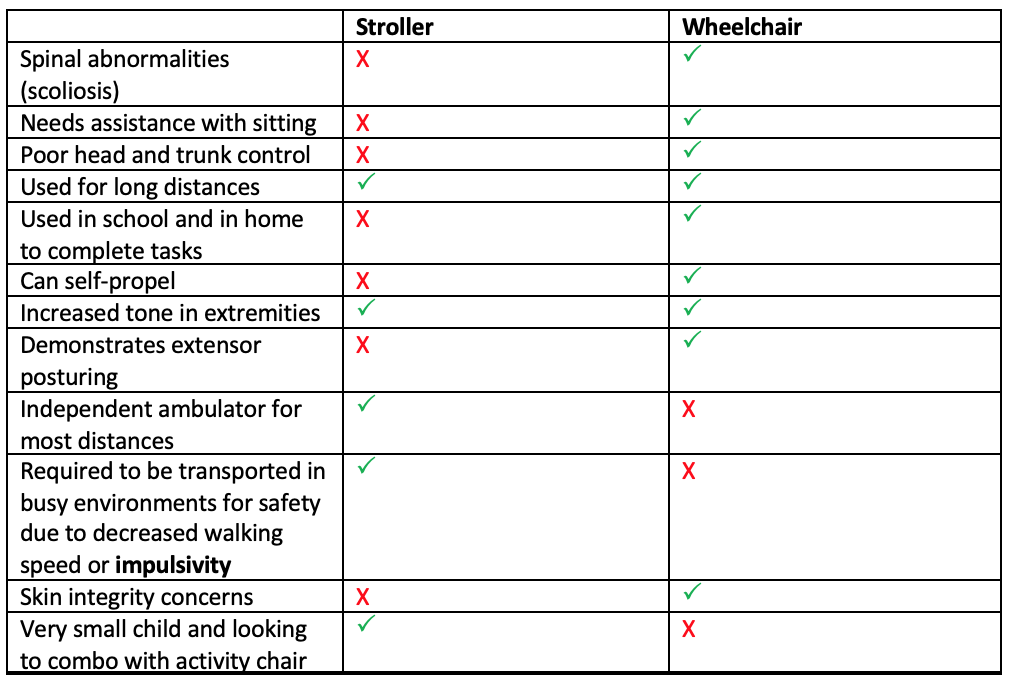
8. Impulsivity and safety concerns
The chart here is only to be used as a visual of the information provided above. All children are different and not every situation is the same. Please use this information to guide your decision and to ask more questions.

Least costly alternative
Comes in 4 sizes: 12 inches wide to 18 inches wide
Weight capacity: up to 75 pounds to 250 pounds
Product weight of stroller 33 pounds to 36 pounds
Folded length of stroller 45 inches
Accessories: headrest extension, adjustable footplates, anti-tippers, bus tie downs, head block, upper extremity support tray, calf panel, ankle positioners, tension adjustable back, canopy, under seat storage
Adjustable back angels: 85, 90 and 95 degrees

Comes in 5 sizes: 10 inches wide to 18 inches wide
Weight capacity up to 250 pounds
30-degree fixed tilt
Approximate product weight: 28 pounds
Accessories: headrest, transit option, harness, foot positioners, canopy, under seat storage

Available in one size
Maximum weight capacity is 110 pounds
Seat width is 14 inches
Weight of the stroller is 27 pounds
Can be adjusted to 50-degree angel for relaxed position
Optional Soft Touch Liner can be added to provide additional lateral and pelvic support
These liners can be removed and used in other Special Tomato products (like the Soft Touch Sitter)
Accessories: head support, harness, canopy and storage bag.

Tilt in space stroller
Recline up to 170 degrees
Allows for reverse seating (so child is facing you)
Maximum weight capacity is 110 pounds
The Stingray Seating System can be used on the Trekker frame for a smaller child up to 88 pounds
The seating system can be removed and placed on high-low indoor frame to double as an activity chair
Lateral trunk and hip support
Accessories: canopy, upper extremity support tray, IV pole, oxygen tank holder, ventilator tray, under seat storage, transit option, harness, foot positioners, pommel





Sample letters of medical necessity
Examples from websites
Medicaid general guidelines
There is no specific information for a stroller. Remember a stroller and a manual wheelchair are coded the same!
Medicaid wheelchair seating and assessment guide
Manual wheelchairs are covered when:
Criterion 1, 2, 3, 4, and 5 are met; and
Criterion 6 or 7 is met, and
Criterion is met for specific devices listed below:
1. The member has a mobility limitation that significantly impairs his/her ability to participate in one or more MRADL, and
2. The member’s mobility limitation cannot be sufficiently resolved by the use of an appropriately fitted cane or walker, and
3. The manual wheelchair supplied to the member for use in the home and/or community settings provides adequate access to these settings (e.g., between rooms, in and out of the home, transportation and over surfaces), and
4. Use of a manual wheelchair will significantly improve the member’s ability to participate in MRADLs and the member will use it on a regular basis, and
5. The member has not expressed an unwillingness to use the manual wheelchair that is provided, and
6. The member has sufficient upper extremity and/or lower extremity function and other physical and mental abilities needed to safely self-propel the manual wheelchair during a typical day. Limitations of strength, endurance, range of motion, or coordination, presence of pain, or deformity or absence of one or both upper extremities are relevant to the assessment of upper extremity function, or
7. The member has a caregiver who is available, willing, and able to provide assistance with the wheelchair.
8. A description of, and cost quote for all the equipment and components as ordered (e.g., HCPCS code, make, model, size, seat and back dimensions) and how they accommodate relevant member measurements (e.g., height, weight, chest, shoulders, thighs, legs).
9. A statement of the alternatives considered or attempted (e.g., manual versus power, single versus multiple power option) and why these alternatives do not meet the member’s medical needs. Least costly alternatives and why they were ruled out.
10. A description of the customary environment and caregiver supports (e.g., skilled nursing facility, OMRDD-certified residence, private home, home health or waiver services); please give details of the results of trial of equipment in this environment (e.g., fitting through doorways, access to home, transportable, ability to safely operate, secure storage space).
11. The practitioner must document medical necessity, to the extent required by the coverage criteria for the specific WME/SPC; how the member’s medical condition supports Medicaid reimbursement.
12. The documentation must be summarized and forwarded to the supplier in the form of a qualified practitioner’s letter of medical justification, an evaluation template and/or, physician's office records, hospital records, nursing home records, home health agency records, records from other healthcare professionals and test reports.
13. The practitioner must maintain appropriate and complete medical records even if a letter of medical justification or evaluation template is provided to the supplier.
Examples of medical documentation which is applicable include but are not limited to:
Explain history of decubitus/skin breakdown, if applicable, how long the condition has been present, Clinical progression, Interventions that have been tried and the results
Past use of walker, manual wheelchair, POV, or power wheelchair and the results
A list of all current WME and SPC (e.g., make, model, serial number, age) and an explanation of why it no longer meets the member’s medical needs (suppliers must obtain cost estimates of repair of equipment)
Reports of pertinent laboratory tests, x-rays, and/or other diagnostic tests (e.g., pulmonary function tests, cardiac stress test, electromyogram, etc.) performed in the course of management of the member 5. Describe other physical limitations or concerns (e.g., respiratory)
Describe any recent or expected changes in medical, physical, or functional status
Related diagnoses
Impairment of strength, range of motion, sensation, or coordination of arms and legs, presence of abnormal tone or deformity of arms, legs, or trunk, posture and flexibility, sitting and standing balance, measurements of height, weight, chest, shoulders, hips, legs, absent or impaired sensation in the area of contact with the seating surface
Physicians shall document the examination in a detailed narrative note in their charts in the format that they use for other entries. The note must clearly indicate that a major reason for the visit was a mobility examination
Describe MRADL capabilities and any problems with performing MRADLs, including the need to use a cane, walker, or the assistance of another person
Describe activities, other than MRADLs, performed while in wheelchair
Transferring between a bed, chair, commode, toilet and WME
Walking around customary environment – provide information on distance walked, speed, and balance
Ability to carry out a functional weight shift
Describe in detail any significant postural asymmetries with applicable quantitative measurements (e.g., scoliosis leg length discrepancy)
Describe feeding capabilities and seating modifications required to facilitate feeding capabilities 16. Specifics why less costly alternatives are not medically appropriate based on the member’s medical needs Plan of Care:
Intended use and amount of time daily the equipment is used and, degree of ambulation in customary environment
What MRADLs will the member participate in with the new WME and SPC
A narration of medical necessity for the WME and SPC, describing what medical needs specific to the member will be met if the equipment is provided.
An estimate of how long the equipment will be needed
If surgery is anticipated, indicate the CPT Procedure code(s) and ICD Diagnosis code(s) and expected surgery date.
Describe anticipated modifications or changes to the equipment within the next three years
Describe the growth potential of the requested equipment in number of years
For SPC, describe whether it can be integrated into a new or existing wheelchair
For members who receive a Group 2 Single Power Option or Multiple Power Options PWC, any Group 3 or Group 4 PWC, or a push-rim activated power assist device, the evaluation must provide detailed information explaining why each specific option or accessory is needed to address the member’s mobility limitation.
Prior to or at the time of delivery of a MWC, POV, or PWC, the supplier, practitioner, or case manager must perform an on-site evaluation of the member’s home to verify that the member can adequately maneuver the device that is provided considering physical layout, doorway width, doorway thresholds, and surfaces. The evaluation should also include a description of the secure storage space in the member’s home for the wheeled mobility device. Whether the WME is approved for the home and/or community, the WME provided must have an accessible secure storage space in the home. A written report of this evaluation should be available on request.